
More Information
Submitted: November 14, 2023 | Approved: November 14, 2024 | Published: January 05, 2024
How to cite this article: Shweta A, Vikas K, Choudhary E. An Unusual Case of Hydatid Cyst Presenting as Pyopneumothorax. J Pulmonol Respir Res. 2024; 8: 001-002.
DOI: 10.29328/journal.jprr.1001050
Copyright License: © 2024 Shweta A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

An Unusual Case of Hydatid Cyst Presenting as Pyopneumothorax
Anand Shweta1*, Kumar Vikas2 and Choudhary Eblow3
1Specialist, Department of Pulmonary Medicine, Burari Hospital, New Delhi, India
2Senior Resident, Department of Pulmonary, Critical Care & Sleep Medicine, AIIMS, Chhattisgarh, India
3Senior Resident, Department of Pulmonary Medicine, Burari Hospital, New Delhi, India
*Address for Correspondence: Anand Shweta, Specialist, Department of Pulmonary Medicine, Burari Hospital, New Delhi, India, Email: [email protected]
A 10-year-old male child presented to the Department of Respiratory Medicine in March 2017, with complaints of dyspnea (mMRC grade 1) for last 14 months which aggravated on right lateral position, left-sided chest pain for 1 year and mild fever for 3 months. There was no hemoptysis, wheeze, and expectoration. The patient gave a past history of straw-colored pleural fluid aspiration one year ago which was diagnosed as tubercular hydropneumothorax (Figure 1)
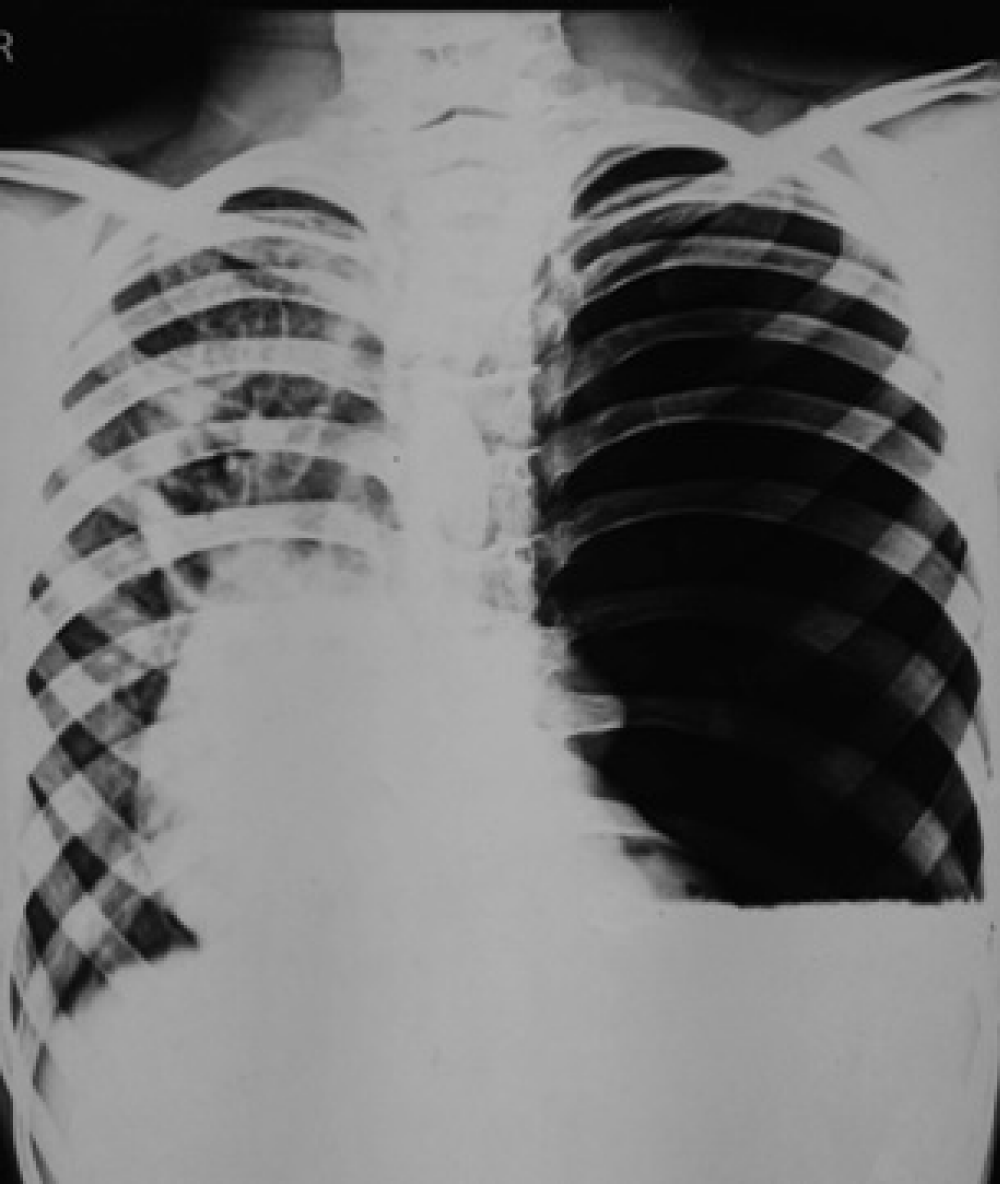
Figure 1: Chest X-ray postero anterior view dated 2016 showing left hydro-pneumothorax occupying the entire hemithorax.
in 2016 based on pleural fluid analysis. He was given antitubercular treatment for the effusion. He took ATT for 8 months but with no improvement.
Currently on examination, the patient was tachypneic, oxygen saturation was 98% at room air, had no peripheral lymphadenopathy, and respiratory movement was decreased on the left side with trachea and apex beat shifted to the right. On the left hemithorax percussion notes were dull and no breath sounds were appreciated. X-ray chest showed left-sided hydropneumothorax with an undulated margin (Figure 2). After informed consent from the patient’s parent, the inter-costal tube was inserted which yielded about 800 ml of pus. Pus was sent for mycobacterial and pyogenic culture and Acid-Fast Bacilli (AFB) smear all of which were negative. A computed tomography chest (Figure 3) was done which showed a hydatid cyst with daughter solices. Hydatid serology came back positive.
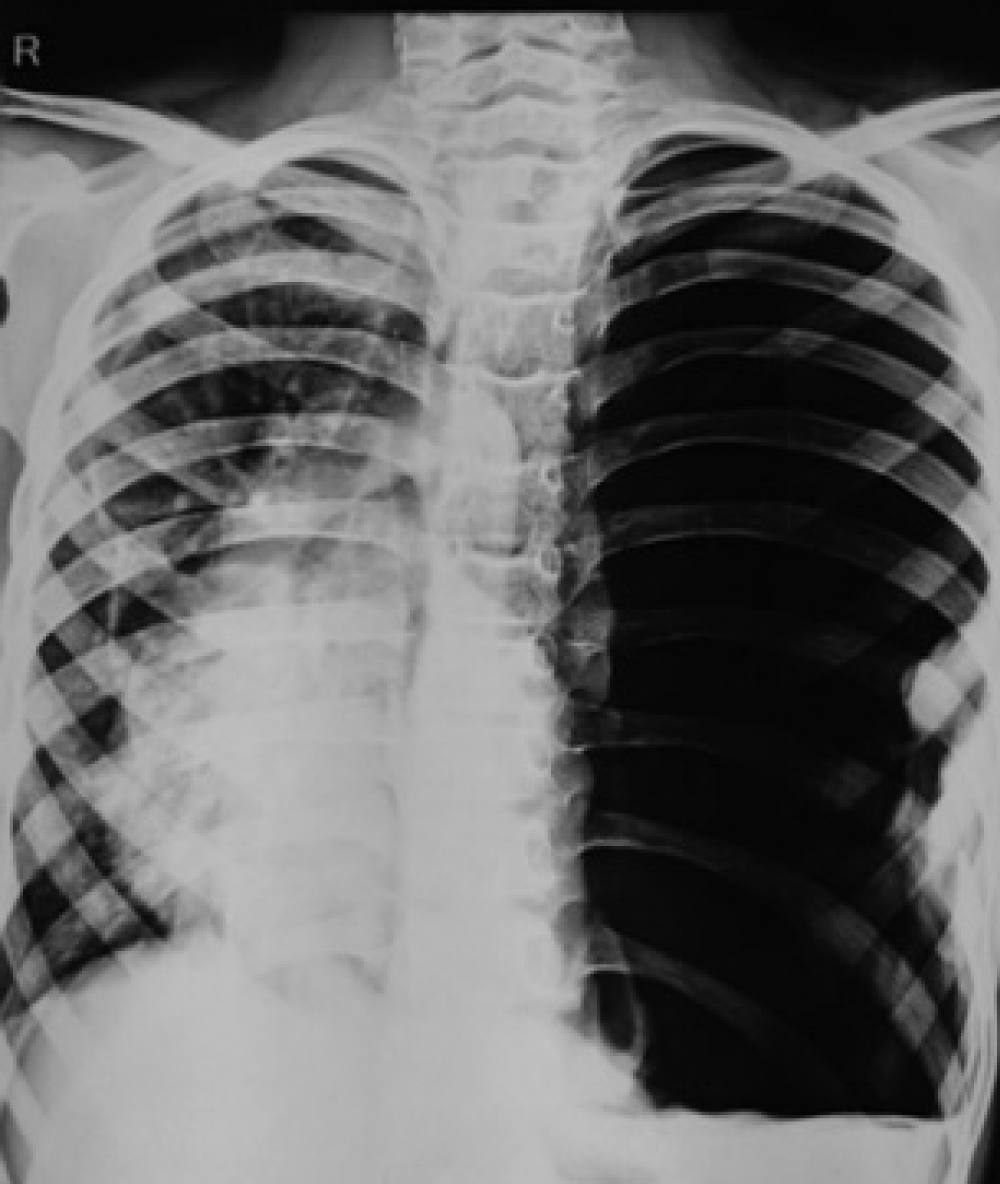
Figure 2: Chest X-ray postero anterior view at the time of presentation dated 2017 showing left hydropneumothorax occupying the entire hemithorax with an undulating margin.
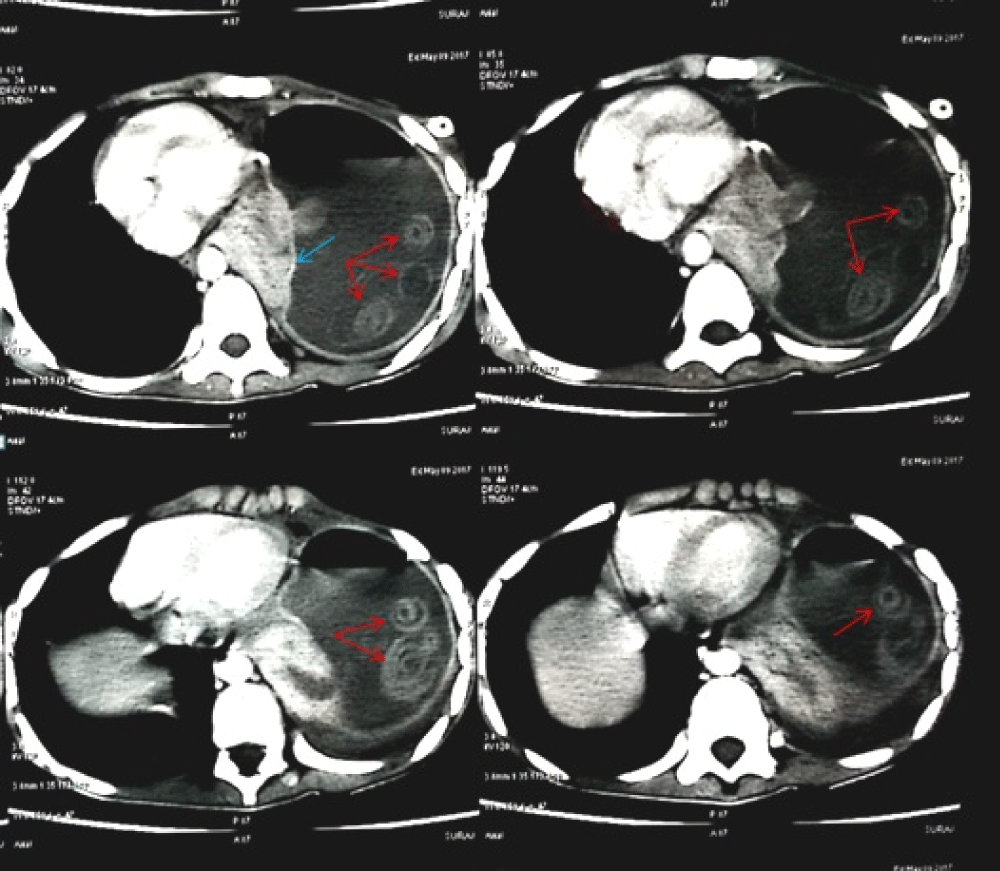
Figure 3: Computed tomography chest showing hydatid cyst with its membranes and daughter solices and collapsed lung.
A diagnosis of hydatid cyst in pleural space complicating into pyopneumothorax was made and the patient was referred to the Thoracic Surgery Department for surgical management. An intrapleural cavity is one of the unusual sites for extrapulmonary hydatid cysts and cysts at this site can rupture and lead to hydropneumothorax or pyopneumothorax.